
If you’ve ever engaged in your own debate or watched one evolve, there are three core pillars of conducting a skilled debate that have stood the test of time:
- Bridge: Finding a common ground, even one point of agreement, is an effective way to build a rapport with the person with whom you are debating. It establishes respect and suggests that the two sides are, perhaps, not as contrarian as might appear on the surface.
- Foundation: A rational, logical point-of-view (POV) starts from a solid & clear foundation, whereas a position based on a weak foundation can usually be unwoven by a simple analogous situation. It is always entertaining to watch a debater coming from a weak foundation trying to execute mental backflips to support a position. This is also where you will see the inherent biases show in a debate.
- Focus on the Topic: Good debaters remember the debate is about supporting an issue or dismantling the credibility of a position, and never make the debate about attacking the person. A methodical review of quality evidence in support of a position will always prevail over an emotional, petulant response. In fact, the weakness in a debate position, and often in the debater, is directly proportional to the emotional petulance exhibited. In other words, the more that someone reverts to name-calling and insults, the weaker their position and argument.
We see these three debate pillars play out almost daily in all areas of our life. From political talking heads & “experts,” to sports analysts, to day-to-day interactions in our jobs, and even at home, it’s easy to compare & contrast a quality debater vs. a weak one.
The Debate within Nutrition & Dietary Lifestyles
In the area of nutrition & dietary lifestyles, we are engaged in a relentless debate. On the one hand (using the above 3 pillars), we have a general agreement that our global population is in a severe state of metabolic sickness. The incidence of type 2 diabetes (T2D), obesity, cardiovascular disease, high blood pressure and a host of other metabolic indicators is too overwhelming for anyone to ignore. On the other hand, however, we are in a serious state of disagreement of HOW to correct this relentless march toward sickness and metabolic disease. Let’s apply our debate filter to a recent article & study of T2D.
Applying our “big 3” pillars mentioned above, we quickly find a common ground around the severity and urgency of the rise in T2D cases. Remember, T2D accounts for 90% – 95% of all diabetes cases, and is not an autoimmune condition, but a metabolic condition that is largely dietary and lifestyle driven. Roughly half-a-billion people across the planet have T2D, more than double the number of people vs. 30 years ago.
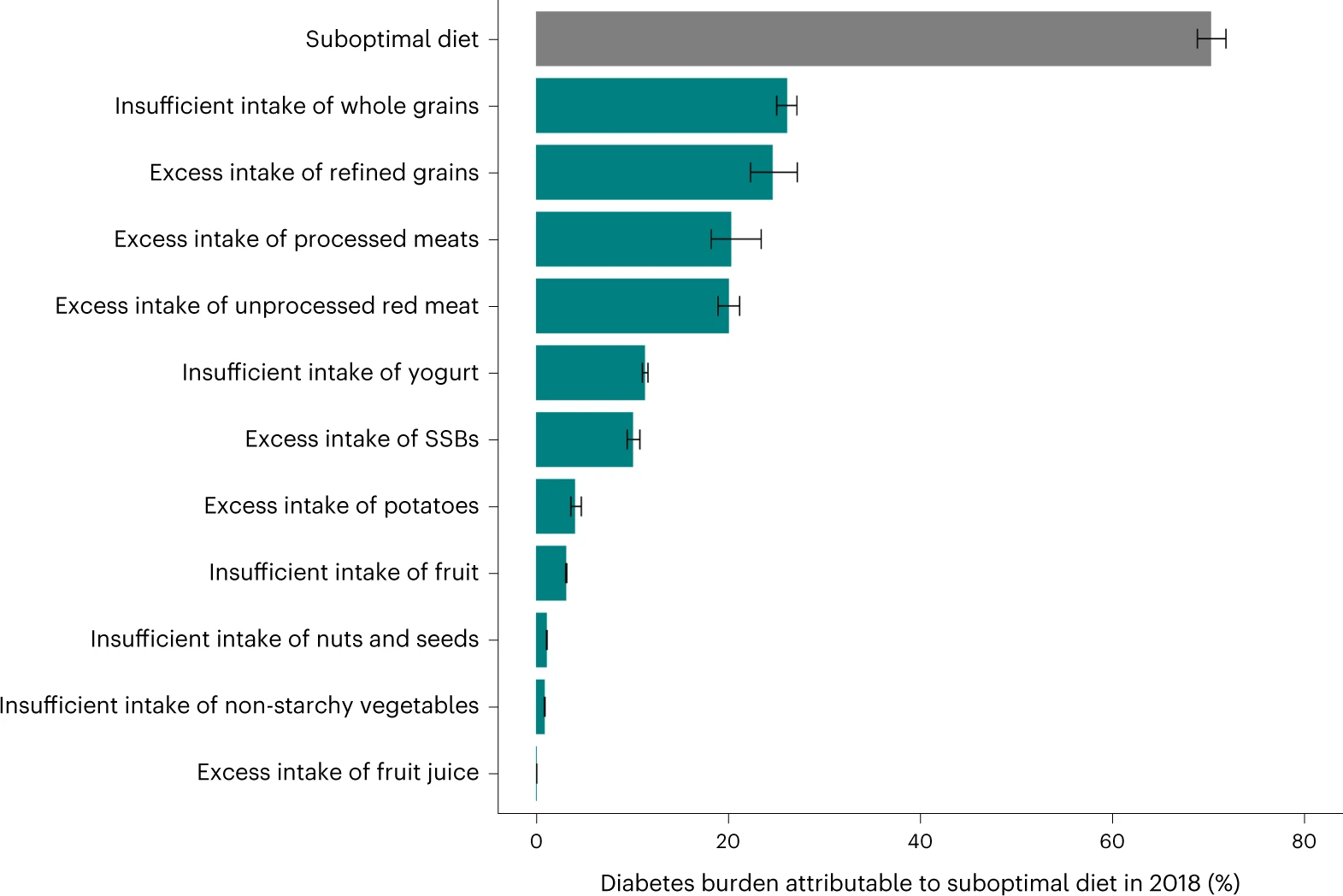
The study & analysis across 184 countries suggests a poor diet was the primary contributor to T2D diagnoses in 2018, highlighting poor diet contributed to over 14M cases, or roughly 70% of the new cases globally in 2018, which is significantly higher than the percentage allocated toward poor diet contribution in previous studies. In fact, from 1990 – 2018, the researchers noted an increase in T2D within every country of the 184 analyzed. Noting a poor diet contributes to T2D is hardly news, but what factors in a diet does the analysis highlight?
The researchers identified 11 different dietary factors and attempted to correlate those 11 factors with the increase in T2D to see if they could associate which factors had the biggest impact. So, what are the 11 dietary factors, why did they choose those, and from what source(s) was the data for the 184 countries?
- The data source(s) came from nutritional survey data. We know survey data, sometimes referred to as epidemiological data, is one of the least reliable methods of epidemiology studies, as it relies on a self-reported set of responses that assume people remember what they’ve consumed, how often, and when. Secondarily, survey data, at its best, can only be correlational, not causal. Correlational means two issues or actions can be related, but one does not necessarily cause another. Causal, on the other hand, is more powerful, as it means one action causes another.
- The 11 key dietary factors (which add up to the “suboptimal diet”) are listed in the graph below. This is one of the first studies to incorporate the refined and whole grains factors.
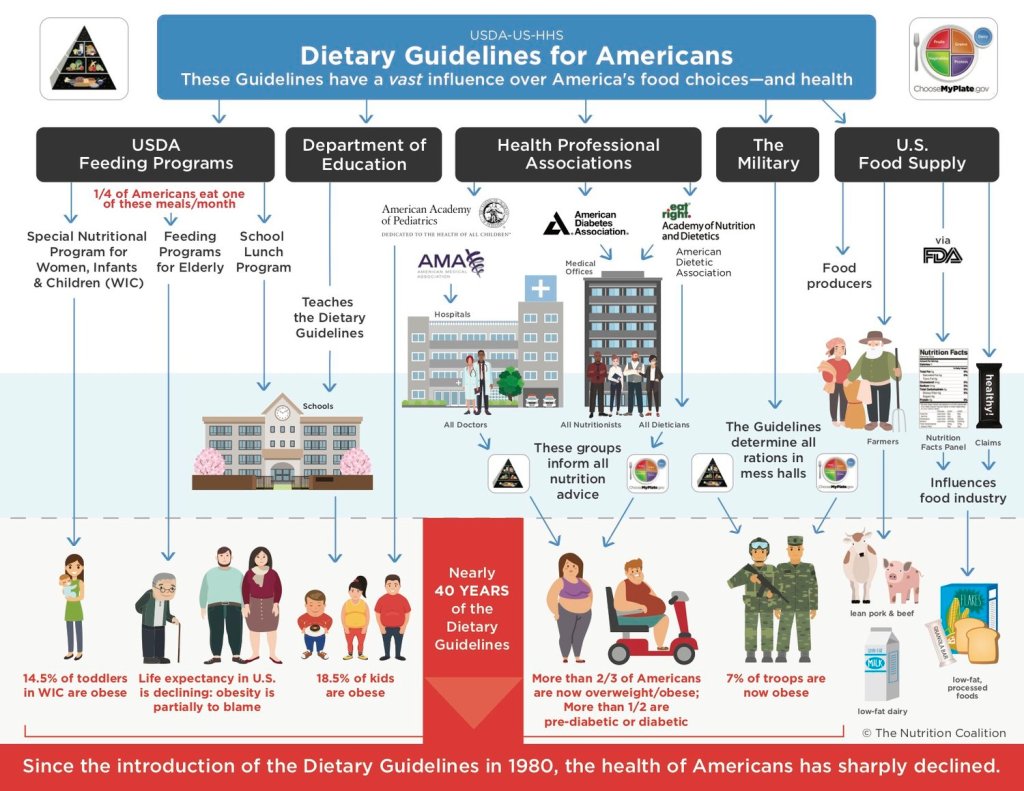
- The study relies on dietary factors from previous studies and currently in-place dietary guidelines. The American Dietary Guidelines (ADG) as an example, have an enormous influence over food choices and health across a wide range of American society, as well as in other parts of the world, as depicted from the image below courtesy of the nutrition coalition. Given the ADG’s recommendation for whole grains, would it be surprising that this report, using guidelines from the ADG, suggests not consuming enough whole grains is a contributor to T2D?
Questioning the Foundation
From a debate standpoint, here’s where this study struggles.
- T2D is a disease of insulin resistance, and the primary driver of insulin secretion and the development of insulin resistance is the copious & frequent consumption of carbohydrates. Other than fiber, which is passed through to the colon, and fructose, which is processed through the liver, any other carbohydrates stimulate insulin, are converted to sugar and stored as glycogen in the body. So, to suggest not eating enough whole grains (carbohydrates) is causing an increase in T2D, metabolically, does not make sense. The researchers also draw no correlation between sugar-sweetened beverages (SSB) and T2D, yet sugary drinks account for almost 1/2 of the added sugars in a standard American diet, and are significant contributors to metabolic disease, including T2D.
- In a similar manner, suggesting unprocessed red meat (which would imply no sugars, nitrates or other fillers) as a direct contributor to T2D does not metabolically make sense. Quality meat, unprocessed, with natural fats, will yield almost no impact on insulin unless it is consumed with carbohydrates. In other words, eating a grass-fed patty with a slice of natural, unprocessed cheese, without anything else, will yield almost no insulin response. However, eating a hamburger, with a bread bun, ketchup and fries, will yield an enormous insulin response. The difference in those two scenarios are the carbohydrates.
- The study presupposes the ADG and World Health Organization (WHO) dietary recommendations are the correct recommendations. However, when you consider the ADG have been formally published since 1980 and ever since we have seen a relentless rise in metabolic diseases, including T2D, it seems highly suspect that these recommendations are the most effective way to achieve metabolic health.
- This study was funded by the Bill and Melinda Gates foundation, which has made huge investments into farming and grain-based diets and also made their drive for the elimination of meat very clear.
In summary, we have less reliable survey data, correlations but no causation, and the recommendations do not make sound scientific sense. We have a presupposition that the ADG are the correct dietary recommendation, which over 40 years of data would suggest is false. Finally, we have a conflict of interest as the recommendations, based only on weak correlational data, happen to match almost perfectly with the source of funding’s drive/investments.
Closing the Debate
It’s sickening how hard the mainstream science and media work to discredit lifestyles and treatments that actually show sound, measurable, demonstrable proof of improving, if not reversing T2D. There was recently another article about how the ketogenic lifestyle is bad for you, as determined by the American Heart Association (AHA), who by the way follows the ADG. Even the AHA article admits the ketogenic lifestyle is helpful and effective in key metabolic areas, but the two things that detract from it are (1) it’s tough to follow and (2) followers can see an LDL cholesterol increase. From the article:
“The AHA noted that while very low carb diets may help with weight loss and improve certain markers of metabolic health, such as blood sugar and triglyceride levels, these effects may be temporary. In fact, these diets can cause an increase in LDL “bad” cholesterol levels, which increases the risk of heart disease.“
Even the Paleo diet, which is not very low carb, is deemed unhealthy by the AHA. Why? It limits grains, fruits, legumes & seed/vegetable oils which the AHA says are imperative for good cardiovascular health. So, which diet does the AHA recommend? The DASH Diet, and there’s a good reason why. The DASH Diet is almost exactly the same as the ADG recommendation, except it places a higher emphasis on sodium reduction.
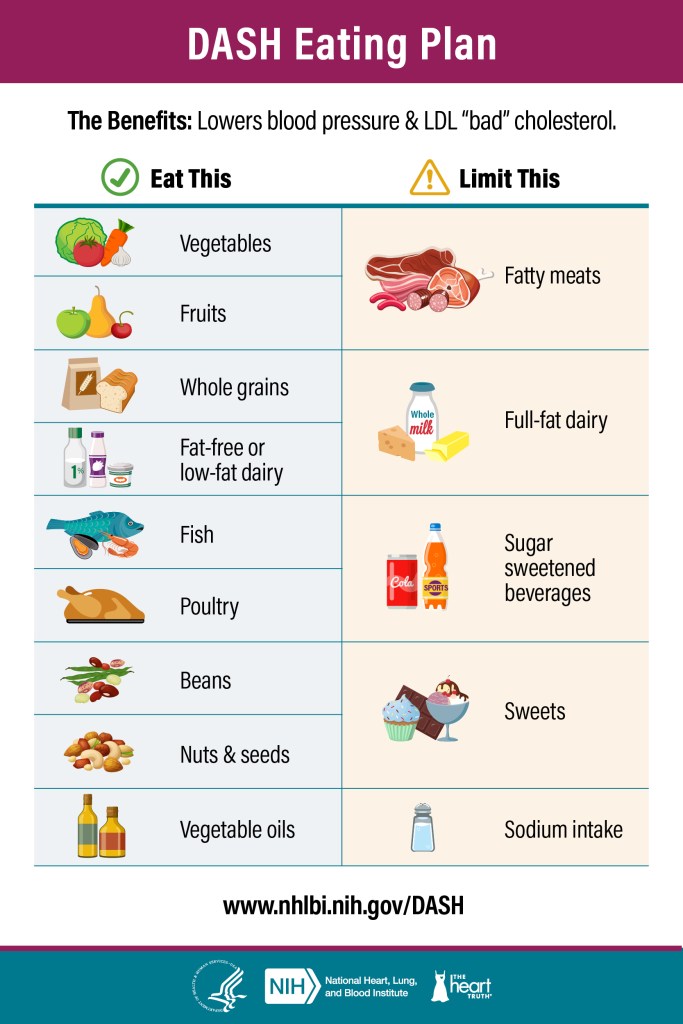
Given the above recommendation, you would think the DASH diet has reams of scientific studies, first class double-blind placebo data, & tightly controlled studies over an extended period of time to confirm this diet is absolutely the best way toward metabolic health. Hardly. In fact, the DASH diet has no long-term studies, and based on a meta-analysis review from Cambridge University Press, the DASH diet has been tested on about 2,000 patients, most of which were middle-aged adults who had hypertension. Oh, and the studies lasted, on the high side, six months. So, based on a poor foundation (the ADG), from which the DASH diet is derived, with no long-term studies and minimal quality research among a niche population, we should follow a recommended dietary plan that, for the last 40+ years has seen the incidence of metabolic disease double across the world?
Compare that to Virta Health’s five-year clinical trial, in a tightly controlled scientific environment, that not only significantly improved metabolic health but in many cases reversed T2D (that means, complete removal from exogenous insulin!), & included both quantitative metrics as well as a range of patients across ages and ethnicities, and the pathway to metabolic health seems pretty clear. As for the mainstream media, how often do we have the same media and scientific community interview Virta Health to discuss their incredible long-term results with patients reversing T2D through dietary and lifestyle changes? Or review the hundreds of positive clinical studies on low-carb diets? Or openly discuss why the ADG are purposely avoiding inclusion of the low-carb diets as an effective way to naturally manage metabolic health? When you look at the evidence, which dietary path to follow to reverse metabolic disease really isn’t a debate.
