
https://hub.jhu.edu/2020/06/01/david-kass-obesity-covid-19/
Have you ever noticed the first question, asked multiple times during a doctor visit, is “are you in any pain?” Doctors are trained to minimize pain and treat the symptoms. If you have not figured it out yet, the U.S. medical system is built upon a “treat the symptoms, not the root cause” philosophy. What do I mean by root cause? Here’s an official definition: A root cause is defined as a factor that caused a nonconformance and should be permanently eliminated through process improvement. The root cause is the core issue—the highest-level cause—that sets in motion the entire cause-and-effect reaction that ultimately leads to the problem(s).
COVID-19 has brought the world to its knees. Health concerns, stories of people suffering and needing a respirator to survive, and a “stop/start” approach from leading medical advisors have enhanced a feeling of helplessness. Part of the reason we have such a disappointing approach to treating COVID-19 is because we are not focused on the root cause. While we have multiple pharmaceutical companies racing to create a vaccine, we are now in “test and treat” mode. Wearing masks may help prevent the spreading of the virus through saliva, breath or a sneeze, and social distancing may help slow down transmission. But these are treating the symptoms. The question we should have answered by now is what are the root causal factors that put people at highest risk of suffering severe symptoms from COVID-19, and how do we address those?
In the attached article from Johns Hopkins University, cardiologist Dr. David Kass talks about their research and findings as they treat COVID-19 patients. To the surprise of exactly no one who has been paying attention to the epidemic in our society, people who are obese are at a higher risk of infection from COVID-19.
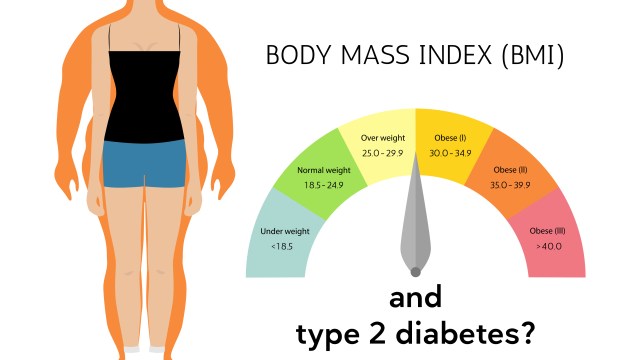
Obesity is defined clinically as a Body Mass Index (BMI) of 30 or more, and those who have a BMI of 40 or more are considered morbidly obese. In the United States, 40% of the population is considered obese.
======================================
COVID-19 Risk Factors From Obesity
Why are obese people more at risk from a viral pathogen like COVID-19? Dr. Kass outlines three likely reasons:
- Hypoventilation. Obesity causes your body to become more inefficient at breathing. Large accumulation of fat below the diaphragm makes breathing more difficult. This is exacerbated as COVID-19 attacks the respiratory system and fluid enters the airway, making it difficult to get oxygen to blood, putting pressure on the diaphragm to work even harder. And this inefficient and underperforming cycle continues to worsen.
- Inflammation. Large accumulation of fat is driven partially by a diet of inflammatory foods, and this fat accumulation also produces pro-inflammatory molecules that build-up in the body. This can include inflammation of the arteries, joints, and organs, as obesity is a key contributor to chronic disease such as heart disease & diabetes. Secondarily, if your body is in an inflammatory state, and a pathogen is introduced, the body’s immune system may overreact, becoming hyperactive and causing even more problems.
- ACE2 Proteins in Fat Cells. Every cell has a lock & key mechanism, and COVID-19 needs this ACE2 protein to enter a cell. Typically, the more fat you have, the more ACE2 you have, which may make your body more susceptible to COVID-19.
Obesity: How Did We Get Here?
The short answer: poor science and political pressure caused our government to make appallingly poor dietary recommendations that set in motion a society that has become more obese, more unhealthy and suffers more chronic disease than at any point in history. Our medical community has been touting the “calories in / calories out” mantra to balance weight and prevent obesity for 50 years, and it has been a dismal failure. It simply does not work.
I recommend you watch the documentary Carb Loaded, and reference my previous blog post for more information. https://wordpress.com/block-editor/post/business-fit.org/699
Below is the My Plate Dietary Guidelines for the United States, led by former First Lady Michelle Obama, and an evolution from the Food Pyramid that so many know from childhood. What do you notice about the macronutrients represented? 75% of the plate is from carbohydrates (which does not even consider the sugar from dairy), and hardly anything from healthy fats.

Talking about the causes of obesity is a very in depth conversation that has been covered in documentaries and books. I recommend The Obesity Code by Dr. Jason Fung as a great read. So, in the spirit of synthesis, in its simplest terms, reversal and prevention of obesity is directly linked to insulin, insulin resistance and the impact on the body’s set weight. Regardless of your sex, race or activity level, if these insulin issues are present, you will be at a higher risk to become obese. So, what can you do starting today to change this trajectory of obesity and the susceptibility to viruses like COVID-19? Make three changes to your diet that will dramatically effect how insulin impacts the body.
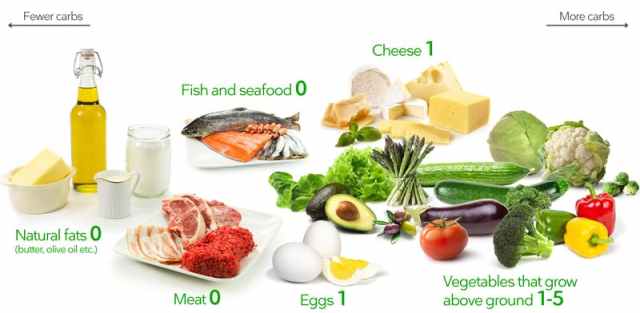
- Quality. Eliminate anything with added sugar, especially soda and sugar juices/drinks. Eliminate processed foods (if it comes in a box or a wrapper and has multiple ingredients, it is likely processed). Eliminate any food that has high fructose corn syrup and dramatically scale back the amount of grain, bread, pasta, fruit and other carbohydrates you are consuming while increasing cruciferous vegetables. Quality protein, quality fat and a robust selection of vegetables that are low on the glycemic index and low on the insulin index are your best choices.
- Quantity. We’re eating between 55% – 75% of our diet from carbohydrates, and carbohydrates are the #1 macronutrient that spikes insulin. Change your quantity to something more like 60% – 70% good fats, 20% – 30% quality protein and 10% carbohydrates. This will take several weeks to re-adjust.
- Frequency. Every time we eat, we spike insulin. The more we snack, the more insulin is secreted, the more fat metabolism is shut off, and the more fat gets stored. The macronutrient that spikes insulin the most are carbohydrates, but even protein will cause a small insulin response (healthy fats cause virtually no insulin response when consumed by themselves). The point is, incorporating intermittent fasting into your dietary plan will go a long way to helping your body change the trajectory toward obesity and insulin resistance. Start with a balanced target of 12/12. That is, eat within a window of 12 hours, then do not eat for 12 hours. Give your body a 12 hour window of no food consumption, and by doing so, you will start to shift from being insulin resistant and constantly adding calories through consumption, to enabling your body to re-balance insulin (thus, achieving insulin sensitivity, which is what we want) and turning to body fat stores for energy. As this occurs, your BMI will begin to drop.

Pingback: Researching the Link Between Leptin & COVID-19 – BusinessFit